Breast cancer characteristics

The cancer will also be tested for a number of other characteristics that can help your doctors decide how it is likely to respond to particular kinds of treatment or how aggressive it may be. These include:
Hormone receptivity. These tests determine whether the cancer cells contain estrogen and/or progesterone receptors. Those that do may respond well to hormone therapies that block the production of female hormones in the body. Learn how hormone therapy works to treat hormone-receptive breast cancers.
Tumor-marker testing/immunohistochemistry (IHC). Also known as human epidermal growth factor 2, or c-erB-2, Her2/neu is a protein necessary for normal cell growth. However, some cancers — including some breast cancers — produce too much of this protein.
High levels of HER2/neu often mean that a tumor is more aggressive, and may respond differently to certain cancer treatments. For example, women with high levels of HER2/neu may be good candidates for certain biological therapies. Learn more about biological therapies in breast cancer treatment.

What is the histological grade of the breast cancer?
Histology is the study of tissues, including cellular structure and function. Pathologists assign a histological grade to a patient’s breast tumor in order to identify the type of tumor present. A pathologist determines a cancer’s histological grade by examining the breast cancer cells and their patterns under a microscope. Three features of cells inside a tumor determine the grade of the cancer:
*Frequency (rate) of cell mitosis (i.e.: cell division)
*Percentage of cancer cells containing tubules (tubular structures)
*Change in size and shape of nuclei within cells
Each of these features is assigned a score ranging from 1 to 3. Cell growth that follows a slower, more orderly pattern is considered Grade 1. If cells are multiplying in a faster, more disorganized way, the cell growth grade is labeled Grade 3.
Generally speaking, the lower the histological grade of the breast cancer, the more favorable the outcome. However, tumors that are higher grade tend to be more responsive to aggressive treatments like radiation and chemotherapy than are low-grade cancers.
Is the cancer invasive or non-invasive?
This characteristic is probably the most important, because it largely determines the types of treatment that you will be offered.
Non-invasive or in situ cancers are those that are contained in the breast ducts or lobules. These types of breast cancer have not spread to the surrounding breast tissue. However, breast cancer in situ can develop into a more invasive and, therefore, more serious form of cancer.
If the cancer is invasive, this means it has spread beyond the breast to the surrounding tissue. Because cells from invasive cancers can pass into the bloodstream or lymphatic system and spread to other parts of the body, invasive cancers are considerably more serious than are noninvasive cancers.


One of the defining traits of a breast cancer is whether or not there are receptors for the female hormones, estrogen and progesterone. Your doctor will order a hormone receptor assay, which is a test to determine if the cancer cells are sensitive to estrogen and progesterone. The results are presented in one of three ways:
*The number of cells out of 100 tested that have receptors. The number is stated between 0% (meaning that no cells with receptors were detected) and 100% (meaning that all cells have receptors).
*A number between 0 and 3. A score of 0 means no receptors, whereas a score of 3 indicates a high number of receptors.
*Negative or positive or negative. Negative means that no receptors are present, whereas positive means that receptors are present.
Cancers that are estrogen-receptor positive (ER-positive) tend to grow better in environments with high levels of estrogen. ER-positive cancers tend to respond better to estrogen blocking drugs, such as Tamoxifen. Tamoxifen works by blocking the estrogen receptors on the cancer cells. By blocking the ability of the cancer cells to receive estrogen, Tamoxifen slows down rate of growth of the cancer cells.
If the breast cancer is ER-negative, meaning there are no hormone receptors present, the breast cancer will not be affected by the levels of estrogen and progesterone in your body. If your breast cancer does not test positive for hormone receptors, do not be discouraged. There are many effective treatments for estrogen receptor-negative (ER-negative) and progesterone receptor-negative (PR-negative) cancers.
Do the breast cancer cells have a normal number of chromosomes?
Knowing how many chromosomes are in your breast cancer cells gives your doctor an idea of how fast your tumor is growing. Ploidy is a measurement of the number of chromosomes in cancer cells. Diploid cells in the breast have a normal number of chromosomes. Aneuploid cells in the breast have an abnormal number of chromosomes. The presence of extra chromosomes mean that, as these cells grew faster than normal, mistakes occurred during cell division, leading to an abnormal number of chromosomes in the cells. Breast cancers containing aneuploid cells grow faster than breast cancers containing diploid cells.
Is the breast cancer caused by oncogene overexpression?
Your doctor will also want to measure the amount of proteins being produced by your breast cancer cells. Excessive levels of certain proteins are caused by oncogene overexpression. Oncogenes are genes that regulate the rate of cell growth in the body. Oncogene overexpression means that extra copies of the oncogenes are present in certain cells. When oncogenes malfunction, they trigger an increased production of oncogene proteins, which in turn, cause the rate of cell reproduction to get out of control. Many types of cancer often are the consequence of uncontrolled growth of cells.
Understanding whether or not a cancer is caused by oncogene overexpression helps you and your doctor better determine the best course of treatment. For example, cancer caused by overexpression of the oncogene, HER-2/neu, may respond well to Herceptin, a medicine especially formulated to combat the actions of the HER-2/neu proteins. Also, breast cancers caused by oncogene overexpression may not respond as well chemotherapy with the CMF regimen and the drug, Tamoxifen. Furthermore, breast cancers caused by oncogene overexpression may require a higher dose of chemotherapy with the CAF regimen in order to produce the best results.
Margins of resection?
Doctors use the term margin or margins of resection to refer to the distance between the breast tumor and the edge of the tissue. The margins are measured on all six sides: front and back, top and bottom, left and right. Knowing how close the cancer cells are to the edge of the tissue will help your doctor decide upon the next step in your treatment (i.e.: additional surgery, radiation, etc).
A breast tumor’s margins are labeled in one of three ways depending on the pathologist’s findings:
*Positive Margins, which mean that there are cancer cells beyond the edge of the tissue
*Negative Margins, which mean that no cancer cells have been found in the area beyond the edge of the tumor. A negative margin is one of the terms that is slightly ambiguous, which are perceived differently by different pathologists. Some pathologists label a tumor’s margin “negative” if even one normal cell is found between the cancer cells and the edge of the tissue. Other pathologists believe that there most be at least 2 millimeters between the cancer cells and the edge of the tissue for a margin to be labeled “negative.”
*Close Margins, which means that the tumor’s margins are neither negative nor positive,
but somewhere in-between a negative and positive classification.
What percentage of the breast cancer cells are reproducing and forming new cells?
Your doctor may order tests to determine how fast your breast cancer cells are making new cells. S-phase fraction and Ki-67 are two tests used to measure the rate of cell growth. By understand how fast your breast cancer cells are reproducing, you and your doctor will have a better idea how fast the breast tumor is growing. If more than 6% to 10% of the breast cancer cells are reproducing and forming new cells, then the growth rate of the breast tumor is considered unfavorably high.
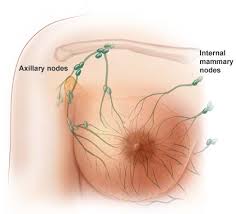
Has the breast cancer spread to the lymph nodes?
In some cases, the breast cancer spreads into the lymph nodes located under a woman’s armpit. Your doctor will examine a sample of your lymph node to see whether or not it contains any breast cancer cells. Lymph nodes that have been invaded with breast cancer cells are called positive lymph nodes. Negative lymph nodes are those that have not been invaded by breast cancer cells.
The number of positive lymph nodes present has been shown to influence the course of the breast cancer. Doctors use one of the following three descriptions to describe the involvement of the lymph nodes:
*Minimal, or microscopic, which means that there are just a few cancer cells in a small number of lymph nodes
*Significant or macroscopic, which indicates that a particular node or a group of nodes have been invaded by cancer cells. These nodes often can be felt under the armpit
*Extra-capsular extension, which means that the breast cancer tumor has completely invaded a lymph node and is spreading to the surrounding fatty tissue
In determining the nature of the breast cancer, the number of positive lymph nodes is more important than the extent to which the breast cancer has spread in a lymph nodes. Most of the time, the more lymph nodes that are involved in the disease, the more aggressive the breast cancer. Doctors use the following categories to describe the lymph node involvement in the breast cancer:
The cancer will also be tested for a number of other characteristics that can help your doctors decide how it is likely to respond to particular kinds of treatment or how aggressive it may be. These include:
Hormone receptivity. These tests determine whether the cancer cells contain estrogen and/or progesterone receptors. Those that do may respond well to hormone therapies that block the production of female hormones in the body. Learn how hormone therapy works to treat hormone-receptive breast cancers.
Tumor-marker testing/immunohistochemistry (IHC). Also known as human epidermal growth factor 2, or c-erB-2, Her2/neu is a protein necessary for normal cell growth. However, some cancers — including some breast cancers — produce too much of this protein.
High levels of HER2/neu often mean that a tumor is more aggressive, and may respond differently to certain cancer treatments. For example, women with high levels of HER2/neu may be good candidates for certain biological therapies. Learn more about biological therapies in breast cancer treatment.
What is the histological grade of the breast cancer?
Histology is the study of tissues, including cellular structure and function. Pathologists assign a histological grade to a patient’s breast tumor in order to identify the type of tumor present. A pathologist determines a cancer’s histological grade by examining the breast cancer cells and their patterns under a microscope. Three features of cells inside a tumor determine the grade of the cancer:
*Frequency (rate) of cell mitosis (i.e.: cell division)
*Percentage of cancer cells containing tubules (tubular structures)
*Change in size and shape of nuclei within cells
Each of these features is assigned a score ranging from 1 to 3. Cell growth that follows a slower, more orderly pattern is considered Grade 1. If cells are multiplying in a faster, more disorganized way, the cell growth grade is labeled Grade 3.
Generally speaking, the lower the histological grade of the breast cancer, the more favorable the outcome. However, tumors that are higher grade tend to be more responsive to aggressive treatments like radiation and chemotherapy than are low-grade cancers.
Is the cancer invasive or non-invasive?
This characteristic is probably the most important, because it largely determines the types of treatment that you will be offered.
Non-invasive or in situ cancers are those that are contained in the breast ducts or lobules. These types of breast cancer have not spread to the surrounding breast tissue. However, breast cancer in situ can develop into a more invasive and, therefore, more serious form of cancer.
If the cancer is invasive, this means it has spread beyond the breast to the surrounding tissue. Because cells from invasive cancers can pass into the bloodstream or lymphatic system and spread to other parts of the body, invasive cancers are considerably more serious than are noninvasive cancers.
One of the defining traits of a breast cancer is whether or not there are receptors for the female hormones, estrogen and progesterone. Your doctor will order a hormone receptor assay, which is a test to determine if the cancer cells are sensitive to estrogen and progesterone. The results are presented in one of three ways:
*The number of cells out of 100 tested that have receptors. The number is stated between 0% (meaning that no cells with receptors were detected) and 100% (meaning that all cells have receptors).
*A number between 0 and 3. A score of 0 means no receptors, whereas a score of 3 indicates a high number of receptors.
*Negative or positive or negative. Negative means that no receptors are present, whereas positive means that receptors are present.
Cancers that are estrogen-receptor positive (ER-positive) tend to grow better in environments with high levels of estrogen. ER-positive cancers tend to respond better to estrogen blocking drugs, such as Tamoxifen. Tamoxifen works by blocking the estrogen receptors on the cancer cells. By blocking the ability of the cancer cells to receive estrogen, Tamoxifen slows down rate of growth of the cancer cells.
If the breast cancer is ER-negative, meaning there are no hormone receptors present, the breast cancer will not be affected by the levels of estrogen and progesterone in your body. If your breast cancer does not test positive for hormone receptors, do not be discouraged. There are many effective treatments for estrogen receptor-negative (ER-negative) and progesterone receptor-negative (PR-negative) cancers.
Do the breast cancer cells have a normal number of chromosomes?
Knowing how many chromosomes are in your breast cancer cells gives your doctor an idea of how fast your tumor is growing. Ploidy is a measurement of the number of chromosomes in cancer cells. Diploid cells in the breast have a normal number of chromosomes. Aneuploid cells in the breast have an abnormal number of chromosomes. The presence of extra chromosomes mean that, as these cells grew faster than normal, mistakes occurred during cell division, leading to an abnormal number of chromosomes in the cells. Breast cancers containing aneuploid cells grow faster than breast cancers containing diploid cells.
Is the breast cancer caused by oncogene overexpression?
Your doctor will also want to measure the amount of proteins being produced by your breast cancer cells. Excessive levels of certain proteins are caused by oncogene overexpression. Oncogenes are genes that regulate the rate of cell growth in the body. Oncogene overexpression means that extra copies of the oncogenes are present in certain cells. When oncogenes malfunction, they trigger an increased production of oncogene proteins, which in turn, cause the rate of cell reproduction to get out of control. Many types of cancer often are the consequence of uncontrolled growth of cells.
Understanding whether or not a cancer is caused by oncogene overexpression helps you and your doctor better determine the best course of treatment. For example, cancer caused by overexpression of the oncogene, HER-2/neu, may respond well to Herceptin, a medicine especially formulated to combat the actions of the HER-2/neu proteins. Also, breast cancers caused by oncogene overexpression may not respond as well chemotherapy with the CMF regimen and the drug, Tamoxifen. Furthermore, breast cancers caused by oncogene overexpression may require a higher dose of chemotherapy with the CAF regimen in order to produce the best results.
Margins of resection?
Doctors use the term margin or margins of resection to refer to the distance between the breast tumor and the edge of the tissue. The margins are measured on all six sides: front and back, top and bottom, left and right. Knowing how close the cancer cells are to the edge of the tissue will help your doctor decide upon the next step in your treatment (i.e.: additional surgery, radiation, etc).
A breast tumor’s margins are labeled in one of three ways depending on the pathologist’s findings:
*Positive Margins, which mean that there are cancer cells beyond the edge of the tissue
*Negative Margins, which mean that no cancer cells have been found in the area beyond the edge of the tumor. A negative margin is one of the terms that is slightly ambiguous, which are perceived differently by different pathologists. Some pathologists label a tumor’s margin “negative” if even one normal cell is found between the cancer cells and the edge of the tissue. Other pathologists believe that there most be at least 2 millimeters between the cancer cells and the edge of the tissue for a margin to be labeled “negative.”
*Close Margins, which means that the tumor’s margins are neither negative nor positive,
but somewhere in-between a negative and positive classification.
What percentage of the breast cancer cells are reproducing and forming new cells?
Your doctor may order tests to determine how fast your breast cancer cells are making new cells. S-phase fraction and Ki-67 are two tests used to measure the rate of cell growth. By understand how fast your breast cancer cells are reproducing, you and your doctor will have a better idea how fast the breast tumor is growing. If more than 6% to 10% of the breast cancer cells are reproducing and forming new cells, then the growth rate of the breast tumor is considered unfavorably high.
Has the breast cancer spread to the lymph nodes?
In some cases, the breast cancer spreads into the lymph nodes located under a woman’s armpit. Your doctor will examine a sample of your lymph node to see whether or not it contains any breast cancer cells. Lymph nodes that have been invaded with breast cancer cells are called positive lymph nodes. Negative lymph nodes are those that have not been invaded by breast cancer cells.
The number of positive lymph nodes present has been shown to influence the course of the breast cancer. Doctors use one of the following three descriptions to describe the involvement of the lymph nodes:
*Minimal, or microscopic, which means that there are just a few cancer cells in a small number of lymph nodes
*Significant or macroscopic, which indicates that a particular node or a group of nodes have been invaded by cancer cells. These nodes often can be felt under the armpit
*Extra-capsular extension, which means that the breast cancer tumor has completely invaded a lymph node and is spreading to the surrounding fatty tissue
In determining the nature of the breast cancer, the number of positive lymph nodes is more important than the extent to which the breast cancer has spread in a lymph nodes. Most of the time, the more lymph nodes that are involved in the disease, the more aggressive the breast cancer. Doctors use the following categories to describe the lymph node involvement in the breast cancer:
No comments:
Post a Comment